Its been just over two years since I was handed a diagnosis of my genetic heart condition known as Long QT Syndrome (LQTS). If you have read the previous post I gave a general description of what it is and where I stood on the subject. Since that time I have been on two medications Nadolol and most recently Propranolol, I was experiencing some side effects and thats why I was changed off the one.
Here is a quick recap, I have Type 3 LQTS – A mutation of the SCN5A (Sodium Channel). I inherited it form my mothers side of the family and the mutations tends to prolong the duration of the ventricular action potential (APD), thus lengthening the QT interval (delayed current). The late current action is due to the failure of the channel to remain inactivated. As a consequence, it can enter a bursting mode, during which significant current enters abruptly when it should not. These mutations are more lethal but less common. This is the point of which I could feel a racing heart or tachycardia.
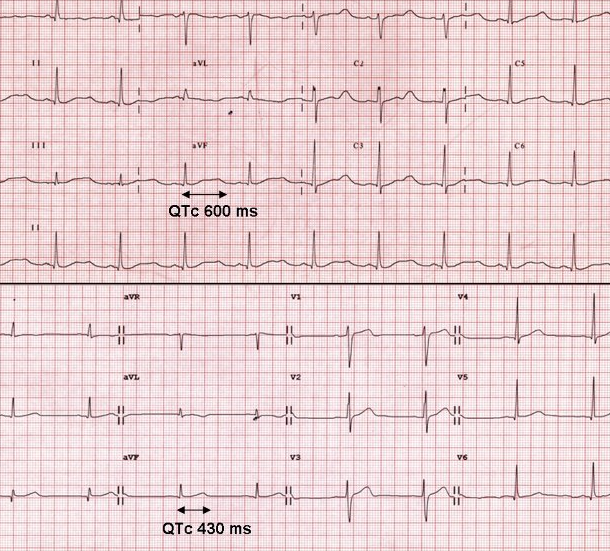
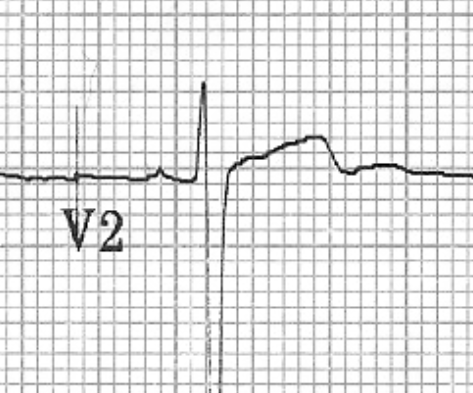
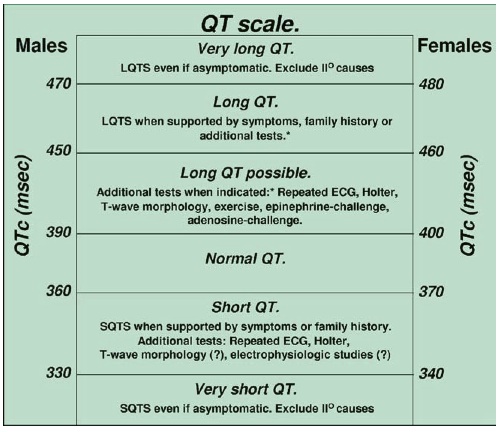 My QT was so pronounced that you could see it on a ECG almost 600msec this is considered beyond “Very long QT” when you consider that normal in an adult male is 360-390msec. Most people with a QT measuring this high are immediately given and Implantable Cardioverter Defibrillator or ICD. Similar to a pacemaker but in the device detects the heart not beating properly or going into tachycardia and shocks it back into normal rhythm. The only reason I do not have one of these is because I have always been and remain asymptomatic to this day.
My QT was so pronounced that you could see it on a ECG almost 600msec this is considered beyond “Very long QT” when you consider that normal in an adult male is 360-390msec. Most people with a QT measuring this high are immediately given and Implantable Cardioverter Defibrillator or ICD. Similar to a pacemaker but in the device detects the heart not beating properly or going into tachycardia and shocks it back into normal rhythm. The only reason I do not have one of these is because I have always been and remain asymptomatic to this day.
This video shows what a life saving tool a ICD can be and more and more you hear of stories like this one.
While I do not have a ICD, with me most of the time is an Automated External Defibrillator (AED) at training session and races alike, just like the ones being installed all over the province in schools and arenas so please check out the Mikey Network and show your support.
Enough about that lets move on.
Both Nadolol and Propranolol are beta-blockers also known as beta-adrenergic blocking agents these drugs specifically block norepinephrine and epinephrine (adrenaline) from binding to beta receptors on nerves.
“Beta receptors are found on cells of the heart muscles, smooth muscles, airways, arteries, kidneys, and other tissues that are part of the sympathetic nervous system and lead to stress responses, especially when they are stimulated by epinephrine (adrenaline). Beta blockers interfere with the binding to the receptor of epinephrine and other stress hormones, and weaken the effects of stress hormones.”
In a nut shell your heart rate drops and with it blood pressure as well. Medications like these are primarily used in people that have any of the following conditions:
- Angina pectoris
- Atrial fibrillation
- Cardiac arrhythmia
- Congestive heart failure
- Essential tremor
- Glaucoma
- Hypertension
- Migraine prophylaxis
- Mitral valve prolapse
- Myocardial infarction
- Phaeochromocytoma, in conjunction with α-blocker
- Postural orthostatic tachycardia syndrome
- Symptomatic control (tachycardia, tremor) in anxiety and hyperthyroidism
- Theophylline overdose
The last words in my previous post I said “I refused to take any suggested medications” well that has obviously changed. I think as part of the diagnosis back in 2013 after all the frustration, anger and sadness had passed I took a step back and thought of the big picture. While doctors tell me I may never have an “episode” anything is possible. Stressing my body and pushing the limits of my heart is something that I do on a regular basis training and racing so better to be safe than sorry.
I started to take Nadolol 40mg/daily and right away I was a zombie…. Nadolol is not a slow release drug and is considered more potent than some other betas. I notified colleagues and close friends that I was not going to be myself for a week or so while my body adjusted to the meds, this adjustment period was difficult because I went from being a semi-hyper individual to a glossy eyed couch potato. I kept as much of a positive attitude as I could while my wife catered to her newly depressed husband, she did everything to keep my spirits up and for that I am forever thankful. The side effects like any medication are long and weird:
Severe allergic reactions (rash; hives; itching; difficulty breathing; tightness in the chest; swelling of the mouth, face, lips, or tongue); behavior changes; blurred vision or other vision changes; burning, numbness, or tingling; fainting; fever, chills, or persistent sore throat; hallucinations; severe or persistent dizziness or light-headedness; short-term memory problems; shortness of breath; slow or irregular heartbeat; sudden, unexplained weight gain; swelling of the hands, ankles, or feet; unusual bruising or bleeding. For me the worst was fatigue, vivid dreams and slow heartbeat.
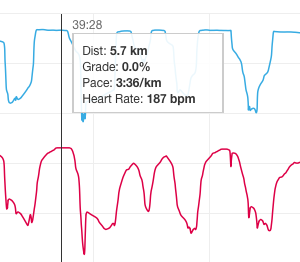
My first race after being on this medication was the Downtown 5K here in London back in 2014, this was going to be a test of what this medication was capable of and how it was going to effect my performance. Anyone who has raced a 5K knows that it is a adrenaline packed all out sprint and with my adrenaline “blocked” no one could predict how my body would react. The result that followed was a shock as I ran a new PB with an all time low HR. As you can see below the data doesn’t lie I ran with an average of 151 bpm. A long way off from 180 + what I was used to.
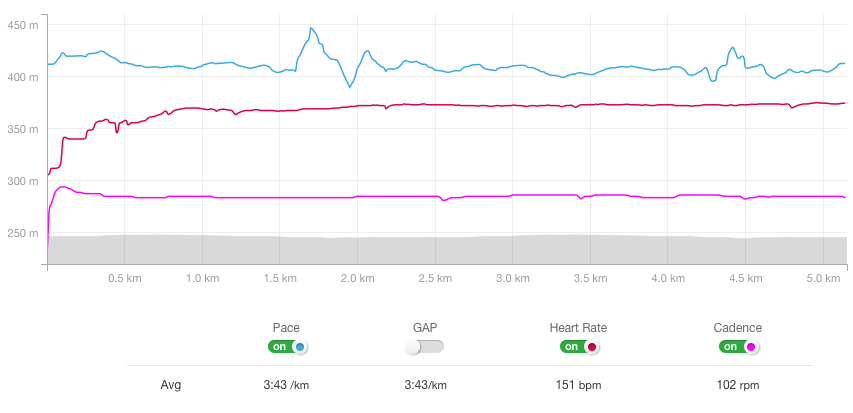
While this was a great result and my time was the best it had ever been I was physically exhausted, not mentally thought I felt almost bored afterwards and wasn’t at all as excited as I should have been…. I remember running the race like I had one speed “on” cadence shows the same story and while some people may think this is cool, it was not… I had discovered that even without my usual adrenaline I could run fairly well but there was this feeling of limitation. This feeling was what is now referred to as my inner “governor” limiting my hearts ability to beat any faster which is NOT a benefit. The largest problem with this was my bodies now limited oxygen supply, and my muscles that seemed to fatigue at an accelerated rate.
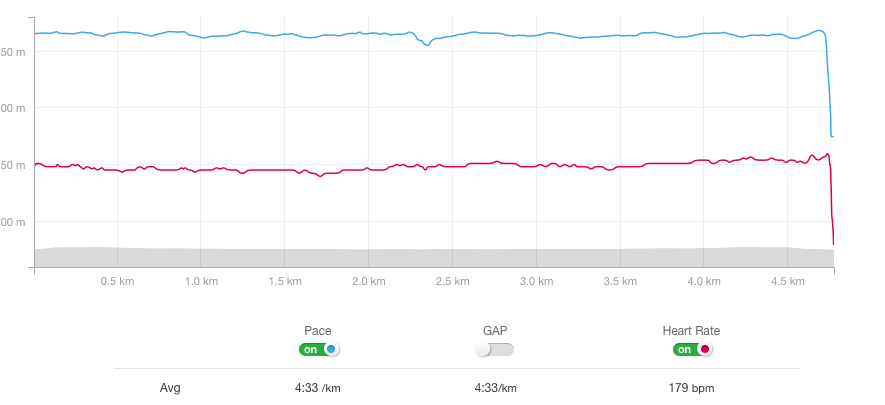
Below is a graph of what my before heart rate looked like with a much higher average. This was from a Duathlon months before going on medication. Some of you may look at this and wonder about pace times, and while my fitness has increased I am showing how this has effected my heart not pace. Pace goes “unaffected” I am just required to work that much harder to maintain my paces. Flushing lactic acid by the way is VERY difficult to do when your muscles are not getting the usual oxygen.
 For all of 2014 I was taking Nadolol and after months and months of hard work I bounced back form my funk and “normal” whatever that was returned to my life. I had a great year of racing and knew that as long as I kept everything in check 2015 would be just as wonderful.
For all of 2014 I was taking Nadolol and after months and months of hard work I bounced back form my funk and “normal” whatever that was returned to my life. I had a great year of racing and knew that as long as I kept everything in check 2015 would be just as wonderful.
This was the plan until I started to experience bouts of large fatigue and a lot of not friendly GI issues…… anyone who runs knows what I am talking about and speed sessions would abruptly have to end. Mostly gas, bloating and diarrhea would ruin my day no matter what I tried. I contacted my cardiologist in Toronto who quickly changed me to a slower releasing beta blocker Propranolol. Through emails back and forth it was determined that sometimes these things just happen and I was in need of a solution asap. We knew it wasn’t exercise related or a food allergy even though it was intense running that amplified the problems so making a simple medication change was all that was needed.
Almost exactly one year after going on Nadolol I switched to the other medication and and all i could think about was that I would go through the same funk and depression I had dealt with a year ago. The one saving grace was that I was instructed to just stop taking my Nadolol and take the Propranolol next day. There was still going to be a withdrawal period but because I didn’t have to taper off the one this made it much easier. Again I notified my colleagues and friends that I could be a zombie for the next week or so while my body transitioned off one medication to another everyone was sympathetic having witnessed me just a year before go through the horror.
The week that followed the switch was not nearly as bad as the first time, for the most part I was just tired really tired like eleven hours a night kind of tired. This combined with an more rigorous raining schedule meant I was out for the count for a while but was still in better spirits compared to the first round. Bouncing back from the fatigue my side effects vanished almost as quickly as they had began, my doctor advised me that it may take some time for them to completely go away but within days my “gut” was back to normal and that helped raise my positivity level tremendously. What I didn’t mention earlier is if you don’t know me I can be a stubborn person, so I had put up with the side effects for two months before doing anything about it…. worst decision ever. I felt like my old self again, I could go for hard runs and not get the runs……… All was returning to normal.
Over the rest of the winter and into this race season I had no issues and am so grateful to have a cardiologist and support team of family and friends that just keep reminding me that “It could be worse”.
I often talk in my race reports about how limited my HR was and I am not a complainer by any means but I truly never know what my heart is going to give me any day of the week. My max HR was 204 bpm before any kind of medication and now I am lucky to get 170+ bpm. Some people have commented saying “must be nice” well let me assure you it’s not. I have the circulation of a 80 year old man and the resting heart rate of an axe murderer 40+.
Naturally I have a heart range of 50-204 bpm, now because of my medication my range is 40-175 bpm. This means I have had to keep my fitness up and train that much harder to get my body moving with less oxygen. My entire heart range shifted down which killed my endurance and is something I still find difficult to deal with at times.
Less oxygen to the muscles equal faster and greater rates of fatigue, I am not saying that a lower heart rate means you are any slower than someone who’s heart beats like a rabbit but for me having to re train my heart after 27+ years of working a certain way has not been a walk in the park.
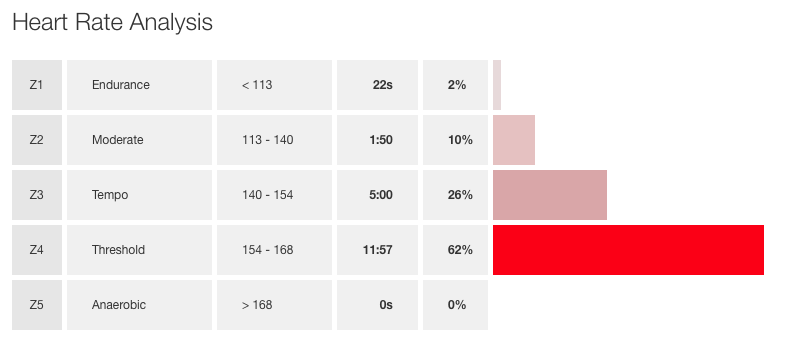
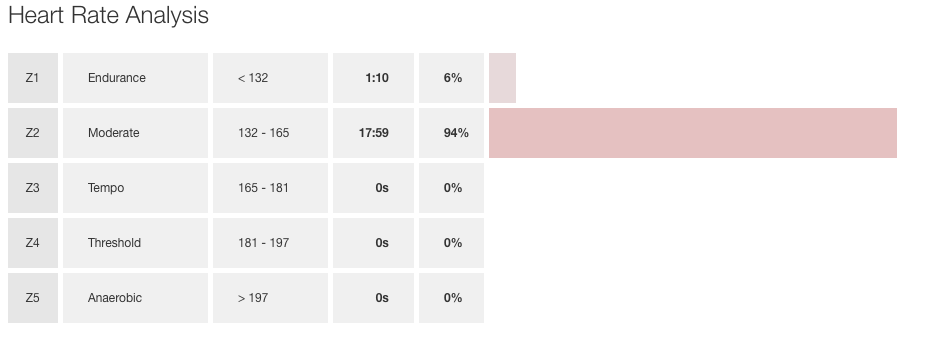
The images below are my heart rate zones from the same race this year a 5K in London. From the first one you can see that most of the time I was racing at threshold 154-168 and that is what I consider normal. When you look at the second image what I have done is adjusted my max HR back to 204 where it used to be and data doesn’t lie Zone 2. If only…. this shows you how much harder my heart is actually having to work to keep up at the same effort level now.
Like any muscle in your body the heart can learn to tolerate less oxygen no matter the demand but this is not something that I have changed overnight and looking to the future there is lots more work to be done. Training sessions can sometimes be great and I might get a lot out of my heart, other days that governor I talked about kicks in and I get nothing form it. I can usually tell during a warmup if I am going to get cooperation from my heart on that given day just by the level it reaches on those first few laps or km’s. If my HR goes to 140 within 10 minutes of warm up I know that it will be a “normal” training session and I will be able to use my full range up to 173 bpm. If it stays down around 80-120…. well then I know it is going to be a slog…
That governor comes into play often and it is right around 160 bpm I can feel it in my chest, at first it was a scary sensation but now I know it is just my heart being limited by my medication. Hard to describe its a pulling sensation or tightening in the chest as the medication reels in the heart……. Think of it like driving a golf cart on the course and you hammer the gas but you get one speed “go forward” you can’t go any faster because they are designed not to, this is how my heart is.
By far my toughest adversary is dealing with the frustration and emotion knowing you are faster but you body is letting you down. I struggle with this constantly and some days are better than others so I take it one day at a time.
If you see me out and about or at a race and want to talk about it please ask me anything, I am an open person and don’t mind talking about all the science stuff!
Just remember if you see me wearing gloves on the hottest day of the summer this is why….low pulse…..


{kind=link}
5 Comments
Darcie · September 19, 2016 at 1:07 pm
Hey Spencer,
Just found your site here as I was searching for info on nadolol and running. My 15 year old daughter runs 5ks for her school’s cross country team. She has LQTS type 2. She has been on nadolol for 2 years. Currently she takes 40 mg every morning.
During 2 races recently, she developed numbness in her feet/legs 800 meters or less before the finish line. She couldn’t walk and it affected her upper body a few minutes later with numbness so her arm/hand muscles were very weak, too. It took 2-3 hours after the unfinished races to regain total sensation and movement. She was dizzy and kept her eyes closed (because she saw double) during those 2-3 hours, also. Thought is was dehydration/heat exhaustion bc they were sunny humid late mornings, but there is more to it.
Questions:
*Did you ever experience any numbness like that on nadolol? Did you take nadolol in the morning or a different time of day?
*I was reading that nadolol’s peak serum concentration (when is hits strongest) is 3-4 hours after taking it (that was when she was racing)
*I’m wondering if she should take the nadolol at night, instead of the morning?
I started thinking about these things today. My daughter has a Dr. appt. tomorrow and we’ll ask these questions there, too.
Thank you for sharing about your sports and LQTS on your site!
Sincerely,
Darcie
Spencer · September 19, 2016 at 1:20 pm
Hi Darcie,
Thanks for reaching out! First sorry to hear about your daughter having this condition as you read I am type 3. While I am no doctor I do know that Type 2 is most at risk with elevated HR and as someone who trains 5-6days a week heavily on running and cycling I do have some thoughts.
I have indeed had numbness and white fingers “raynoids” as a result of such a low heart rate on the betas, mostly tingling in my leg muscles and hands. This would only happen for me while I was undergoing “intense” interval type running. 5K is my favourite distance and for sure she is running all out so I am not surprised she has had issues.
When my HR spikes from a sprint of what have you I could feel the “governor” kick in as it pulled my heart rate down and kept it as a slower rhythm it was a strange feeling that I got used to but when it would happen it was hard to tell if my limbs were numbing or I was getting a “body buzz” from running.
Nadolol does indeed have a peak at 3-4hrs so it never hurst to try and take it the night before with dinner or wait until after the race and take it. There is still enough in your body to do so.
Ask the doctor obviously I am just making suggestions here but I would try night before or after at lunch. Hope you can figure it all out.
P.S.
I have never felt dizzy but muscle weakness is an unfortunate side effect from betas. Ask about “propranolol” its a slow acting beta alternative to nadolol. I went on it for a brief period and it seemed to lessen some side effects. Thanks for reading and please don’t hesitate to email me or write back here if I can help in anyway.
Darcie · September 19, 2016 at 1:47 pm
Thanks for your reply Spencer. I will have to inquire more from my daughter about experiencing that “governor” feeling. It really helps to discuss this with you, as an athlete who has been down this type of road.
When we went to the ER (after her most recent race), the medical staff was helpful, but they don’t get into the details of the side effects of a beta blocker when intensely exercising.
Best wishes in your sports!
Winona Lefebvre-Castillo · February 2, 2020 at 9:47 pm
Hi i’m doing sprints i just started nadolol for LQTS (1 or 2) do y ou think that i’ll be able to do my events.? I’m doing track. 100m to 600m.
Spencer · February 3, 2020 at 9:49 am
From what I know about betas, your heart rate will be limited. That’s what it does. Limited in the sense that your maximal top end will be lower than if you were not taking them. Sprinting is about explosive power and adrenaline. Beta-blockers shut off the body’s ability to make adrenaline, so it will be more challenging. I wish you the best of luck. Don’t let it change you. Before I was on Nadalol my max HR was 195-198 after 3 years of medication and I have since stopped my max HR is only 185. While on betas I was limited to a max HR of 163bpm…. not ideal for speed work. Live your best day every day and push yourself we are all capable of great things.
Comments are closed.